The Feeling-State Theory was developed by Robert Miller, Ph.D.
The Flash Technique was developed by Philip Manfield, Ph.D., and Lewis Engel, Ph.D.
This hybrid protocol combining Feeling-State Theory with the Flash Technique was developed by Joseph Nicolosi Jr., Ph.D.
Introduction
In one sense, a “feeling-state” (FS) is like a trauma. Yet, instead of being a fixated traumatic memory associated with negative emotions (like pain or terror), it is paradoxically associated with fixated positive emotions (e.g., a euphoric rush or intensely feeling “wanted”). A feeling-state is formed when an intense, dysregulating positive experience becomes fused with an action, a person or an object. Unlike typical memories (and much like trauma memories), feeling-state memories are resistant to fading over time and continue to drive compulsive behavior. These fixations bypass rational decision-making, leading to substance addictions or behavioral addictions such as gambling or compulsive sexual behavior. It is thought that FSs develop in response to unmet psychological needs, such as a need for belonging, validation, or control.
Any behavior can be associated with a feeling-state, and the behavior does not have to be intrinsically pathological (e.g., shopping, playing cards or playing video games), but the feeling-state locks the person into a “tunnel vision” in which the individual continues to engage in the behavior compulsively, chasing a good feeling, despite potentially serious consequences or violations of the individual’s own values and goals.
For example, a person may feel deeply accepted and powerful while gambling (positive emotion). This emotional charge becomes fixated with the act of gambling. Over time, gambling is no longer just about money—it is about re-living that powerful feeling over and over again, making it compulsive.
How the Feeling-State Flash Technique (FSFT) works:
The FSFT aims to resolve this fixation by:
- Identifying the FS driving the behavior.
- Processing it using the Flash Technique to reduce its intensity.
- Addressing the underlying negative schema that created the intense desire for the FS.
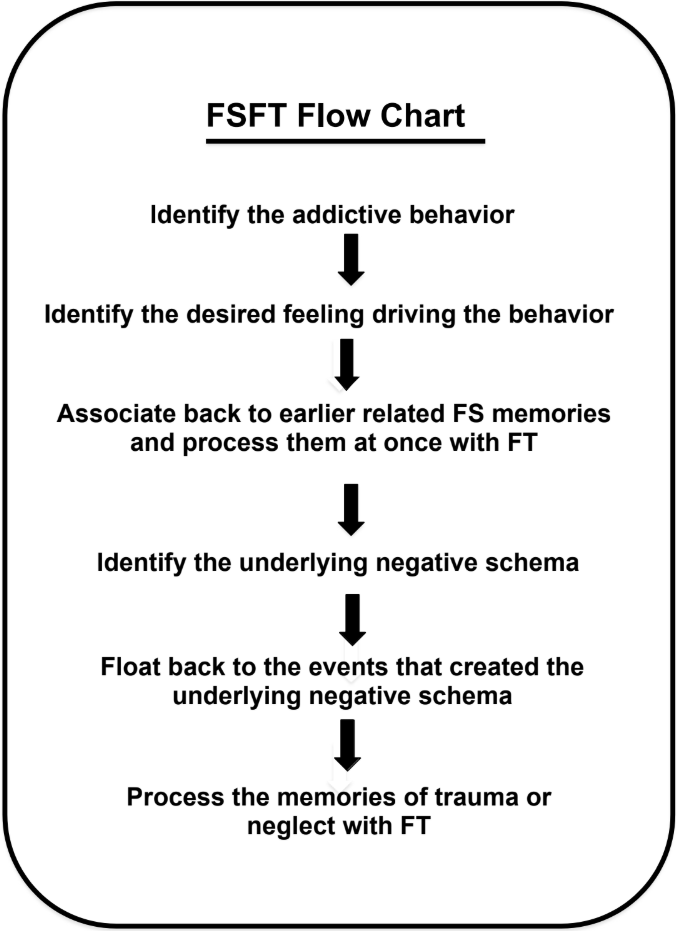
The FSFT Flow Chart
The Feeling-State Flash Technique (FSFT) flow chart illustrates the different steps of the FSFT. The FSFT processes the addictive behavior in the reverse direction in which it was created. Starting with the addictive behavior, it first processes the FS, then identifies the underlying schema, and finally, processes the negative events that created the intense desire for the feeling in the first place. Processing in this order helps reveal how the fixated positive feeling, the negative schema, and the traumas that created that schema are directly related to the addiction.
Processing the FS first allows the underlying negative schema to surface into awareness. In fact, sometimes the trauma begins to emerge before the FS is even completely processed.
The Feeling-State Flash Technique
Words in italics are statements the therapist might make to the client.
Phase 1: History and Evaluation
- Obtain history, frequency, and context of addictive behavior.
- Evaluate whether the person has the coping skills to manage negative feelings without relying on substances. For clients who are too fragile to release the addictive behavior, process their pain, terror, and traumas until they are capable of living without the addictive behavior.
Phase 2: Preparation
- Prepare the person for doing the flash technique.
- Explain the FSFT, including the Feeling-State Theory and how fixated memories cause behavioral and substance addictions.
- Explain how addictive behavior can also be used to avoid re-experiencing negative feelings and memories.
Phase 3: Processing the FS
- Identify the specific aspect of the addictive behavior that has the most intensity associated with it. If the addiction is to a stimulant drug, then the rush/euphoria sensations are usually the first to be processed. However, if some other feeling is more intense, process that first. The starting memory may be the first time or the most recent–whichever is most potent.
- Locate and identify any physical sensations created by the positive feelings. This can be enhanced by asking the client for any sensations he feels within his body, any external sensory information that adds to his positive feelings, such as what he is seeing, hearing, touching, etc. If another person is involved, ask the client for the attitude in the other person that heightens the client’s positive feelings.
- Identify the specific self-referential positive feeling linked with the addictive behavior (e.g., “belonging,” “unstoppable,” “worthy”). Once the client has identified the peak moment of the addictive behavior, and is able to recall that intense feeling as a body sensation, the therapist can inquire, “What is this incredible positive feeling you have about yourself in this moment?” (e.g., important, belonging, euphoric, powerful)
- Measure the intensity of the link between the feeling and the behavior using the Positive Feeling Scale—PFS (0 – 10) scale. The PFS always measures the intensity of this link. (e.g. When you imagine yourself smoking with your buddies, how intensely do you feel that you belong?) Have the client visualize performing the addictive behavior–feeling the positive feeling combined with the physical sensations.
- Ask the client to associate back to an earlier time he had this same kind of experience. If an earlier memory cannot be identified as a clear link to the current memory or fantasy the client has in mind, simply use the current memory or fantasy. If an earlier memory can be identified, process both the early memory and the current memory or fantasy.
- Perform the Flash Technique until the PFS level drops to 0 or 1.
- Ask the client to replay the memory or scene in his mind, and scan his body for any sensations. The client should carefully reassess his internal body sensations, external senses (touch, sound, etc.), and (if applicable) the attitude of the other person that activates his positive feelings. Perform the flash technique until there is no emotional or somatic activation related to the FS.
Phase 4: Process the negative feeling underlying the FS
- Identify the negative schema that underlies the feeling. What’s the negative feeling you have about yourself that makes you feel you can’t (belong, can’t connect, aren’t important, etc.— whichever self-referential feeling the client mentioned in step 7).
- Use the float-back method to identify events related to that negative schema. Can you remember any events that led you to feel that way? If no event is identified, target the body sensation related to the negative schema. Process with the flash technique.
- Install future templates related to the positive cognition of trauma processing.
- Install a positive cognition when the client revisits the original FS-related memory or fantasy. One option that clients frequently find helpful is, “I have other ways of feeling [the original FS name the client chose].”
- In the next session, re-evaluate the addictive behavior for the feeling-state identified in the last session. If that FS is still active, continue processing. If the FS has been eliminated, evaluate for other FSs.
Discussion of the feeling-state flash technique
The FSFT identifies and targets all the elements that must be processed in order to eliminate compulsive behavior resulting from a feeling-state, and processes them using the Flash Technique for faster processing, and for processing multiple memories at once. Because FSs have such destructive influences on a person’s life, eliminating the addiction makes working through other issues easier. Therefore, the treatment should remain focused on processing the FS, even when other issues arise. However, sometimes when processing the FS, the person may begin to associate the feeling-state with traumatic memories. If the person can be sensibly brought back to processing the FS, then the FSFT processing should be continued. Other times, the traumatic memory is too overwhelming and must be immediately worked through. This is not a problem. Divergences from the protocol are common. The FS will still be there waiting to be processed. After working through the trauma with the flash technique, return to the point in the protocol where the divergence occurred and pick up where the FSFT processing left off. Diverging from the protocol when necessary is perfectly acceptable.
Phase 1: This phase has two purposes: first, to establish the general safety of the client for removing FSs. Feeling-states are very powerful dynamics that can serve to temporarily emotionally stabilize a person. When an FS is eliminated, that source of the desired feeling is gone. If a person has no other way to obtain that feeling, he may become depressed or may act out in other ways. Therefore, in Phase 1, the person’s capacity to release FSs needs to be assessed.
For example, if a person has been suicidal because of his destructive gambling behavior, then removing the FS driving the gambling behavior would give the person hope of a better life. On the other hand, if the gambling was more a way to cope with a pre-existing depression that had become at times suicidal, then removing the FS would be contraindicated. In this case, use another treatment to clear the depression and other issues that he has been unable to cope with except by enacting the addictive behavior.
The second purpose of Phase 1 is to get a general history of the person’s addictive behavior–when it began, frequency over the years, periods of abstinence, attempts to quit, etc. This phase also determines whether there is likely to be a co-morbid dynamic such as anxiety or trauma symptoms that may need to be addressed first. If the person has a problem with depression or anxiety that preceded the addictive behavior, those issues may need to be treated prior to focusing on the addictive behavior. The clinical experience of the therapist should guide the appropriate course of treatment.
In Phase 1 another crucial evaluation is made–is the behavior the result of avoiding a feeling or seeking a feeling? The evaluation of the cause of the behavior determines the choice of treatment. If the person is performing the behavior because he is avoiding a feeling, then the appropriate treatment is to process the memories, images, and feelings that the person is avoiding. If the person is performing the behavior in order to experience a feeling, then FS treatment is indicated.
Phase 2: Phase 2 is the preparation phase. The Feeling-State Theory is explained, describing how behaviors can become fixated to desired feelings–the FS. In addition, the possibility that an underlying trauma may surface is explained as well as the use of the flash technique to process the traumatic memories.
Phase 3: Phase 3 gets specific about the addictive behavior. In this phase, the exact dynamics of the behavior, from beginning to end, are identified, as are the feelings associated with the behavior. The purpose is to identify the FS. This can be done by identifying the “peak moment” of the behavior in which the dysregulating/addictive positive affect is the highest. What’s the feeling you get about yourself at this peak moment? (e.g. important, powerful, euphoric, bonded, etc.) By recalling the intense event and recalling the associated dysregulating positive sensations in the body, the client reactivates the target schema so that it can be processed. This should not be done from the client’s head in an intellectual way— the recall of the memory at the peak moment should be “felt” in the body to accomplish this.
Once the FS is identified, process it using the Flash Technique.
Phase 4: In Phase 4 the negative schema underlying the FS is identified. This is a very important step that helps reveal the underlying emotional schema about the client’s self-appraisal that drives his symptoms. The earlier phases of FSFT identified the positive affect of the client in relation to his addictive behavior. From Phase 4 onward, this protocol addresses the negative emotions that the client avoids through his addictive behavior. A floatback is done to identify the events that created the negative schema.
In accordance with the principles of memory reconsolidation, this technique works best when it fully reactivates target schema. This often involves connecting with deeply personal and vulnerable information. When the client can access the nuances of the sensations at the “peak” moment, such as touch taste, sound, etc., this will allow for more powerful and complete processing. For the client who does not feel enough trust with the therapist to discuss such details, this inhibition may prevent him from truly reactivating the target schema— a necessary prerequisite for memory reconsolidation.
Clients do not have to disclose every single detail about the event or fantasy they wish to work on, but they should at least be able to tune into it in their own minds, even if they don’t articulate all the specific details to the therapist. Overwhelming shame can interfere with this. In those cases, the groundwork for a deeper, accepting therapeutic relationship may have to be developed first, before FSFT is employed.
I want you to go back to that memory and carefully see if you can identify what aspects of it still activate that feeling in you. Scan your body from head to toe. Are there any body sensations left in you? Take a moment to sit with that memory. Are there any sounds, touch, smell or taste sensations from this image that still activate a feeling in you? Is there an attitude from this other person that can still activate that feeling in you?
When recalling the peak moment, assess three categories: 1) the client’s own body sensations, 2) the 5 senses that become active, and 3) if another person is present, that other person’s attitude toward the client that activates the feeling-state. Even several minutes of flash technique can lead the client to report that he doesn’t really care about the details of the scene in the same way he first did. Those nuances often remain, and are not consciously accessible to the client until he is prompted to take his time to really check for them. That is why carefully re-assessing the memory can help reactivate the target schema so that complete reprocessing can be achieved.